Knee
Anatomy

The knee is a complex joint made up of different structures including bones, tendons, ligaments and muscles. They all work together to maintain normal function and provide stability to the knee during movement.
Having a well-functioning healthy knee is essential for our mobility and ability to participate in various activities. Understanding the anatomy of the knee enhances your ability to discuss and choose the right treatment procedure for knee problems with your doctor.
Bones
The Knee is a hinge joint made up of two bones, the thigh bone (femur) and the shinbone (tibia). There are two round knobs at the end of the femur called femoral condyles which articulate with the flat surface of the tibia called the tibial plateau. The tibia plateau on the inside of the leg is called the medial tibial plateau, and on the outside of the leg it is called the lateral tibial plateau.
The two femoral condyles form a groove on the front (anterior) side of the knee called the patellofemoral groove. A small bone called the patella sits in this groove and forms the knee cap. It acts as a shield and protects the knee joint from direct trauma.
A fourth bone called the fibula is the other bone of the lower leg. This form a small joint with the tibia. This joint has very little movement and is not considered a part of the main joint of the knee.
Articular Cartilage and Menisci
Movement of the bones causes friction between the articulating surfaces. To reduce this friction, all articulating surfaces involved in movement are covered with a white, shiny, slippery layer called articular cartilage. The articulating surface of the femoral condyles, tibial plateaus and the back of the patella are covered with this cartilage. The cartilage provides a smooth surface that facilitates easy movement.
To further reduce friction between the articulating surfaces of the bones, the knee joint is lined by a synovial membrane which produces a thick clear fluid called synovial fluid. This fluid lubricates and nourishes the cartilage and bones inside the joint capsule.
Within the knee joint between the femur and tibia there are two C shaped cartilaginous structures called menisci. Menisci function to provide stability to the knee by spreading the weight of the upper body across the whole surface of the tibial plateau. The menisci help in load bearing by preventing the weight from concentrating onto a small area, which could damage the articular cartilage. The menisci also act as a cushion between the femur and tibia by absorbing the shock produced by activities such as walking, running and jumping.
Ligaments
Ligaments are tough bands of tissue that connect one bone to another bone. The ligaments of the knee function to stabilize the knee joint. There are two important groups of ligaments that hold the bones of the knee joint together, collateral ligaments and the cruciate ligament.
Collateral ligaments are present on either side of the knee. They function to prevent the knee from moving too far during side to side motion. The collateral ligament on the inside is called the medial collateral ligament (MCL) and the collateral ligament on the outside is called the lateral collateral ligament (LCL).
Cruciate ligaments- This group of ligaments, present inside the knee joint, control the back and forth motion of the knee. The Cruciate ligament in the front of the knee is called anterior cruciate ligament or ACL and the cruciate ligament in the back of the knee is called posterior cruciate ligament or PCL.
Muscles
Muscles: There are two major muscles, the quadriceps and the hamstrings, which enable movement of the knee joint. The quadriceps muscles are in the front of the thigh. When the quadriceps muscles contract, the knee straightens. The hamstrings are in the back of the thigh. When the hamstring muscles contract, the knee bends.
Tendons
Tendons are structures that attach muscles to the bone. The quadriceps muscles of the knee meet just above the patella and attach to it through a tendon called the quadriceps tendon. The patella further attaches to the tibia through a tendon called the patella tendon. The quadriceps muscle, quadriceps tendon and patellar tendon all work together to straighten the knee. Similarly, the hamstring muscles at the back of the leg are attached to the knee joint with the hamstring tendon.
Conditions
 Knee Pain
Knee Pain Anterior Knee Pain
Anterior Knee Pain-
 Runner's Knee
Runner's Knee -
 Osgood Schlatter Disease
Osgood Schlatter Disease -
 Chondromalacia Patella
Chondromalacia Patella -
 Jumper’s Knee
Jumper’s Knee -
 Bursitis
Bursitis -
 Baker’s Cyst
Baker’s Cyst -
 Iliotibial Band Syndrome
Iliotibial Band Syndrome -
 Lateral Patellar Compression Syndrome
Lateral Patellar Compression Syndrome -
 Osteochondritis Dissecans
Osteochondritis Dissecans -
 Shin Splints
Shin Splints -
 Knee Injury
Knee Injury -
 Unstable Knee
Unstable Knee -
 Goosefoot Bursitis of the Knee
Goosefoot Bursitis of the Knee -
 Knee Sprain
Knee Sprain -
 ACL Tear
ACL Tear -
 MCL Tear
MCL Tear - MCL Sprain
-
 Meniscal Injuries
Meniscal Injuries -
 Meniscal Tears
Meniscal Tears -
 Ligament Injuries
Ligament Injuries - Multiligament Instability
-
 Knee Arthritis
Knee Arthritis -
 Patellar Dislocation/Patellofemoral Dislocation
Patellar Dislocation/Patellofemoral Dislocation -
 PCL Injuries
PCL Injuries - Chondral (Articular Cartilage Defects)
-
 Patellar Instability
Patellar Instability -
 Patellofemoral Instability
Patellofemoral Instability -
 Patella Fracture
Patella Fracture - Recurrent Patella Dislocation
-
 Quadriceps Tendon Rupture
Quadriceps Tendon Rupture -
 Patella Tendon Rupture
Patella Tendon Rupture - Lateral Meniscus Syndrome
- Medial Meniscus Syndrome
-
 Tibial Eminence Spine Avulsions
Tibial Eminence Spine Avulsions -
 Osteonecrosis of the Knee
Osteonecrosis of the Knee -
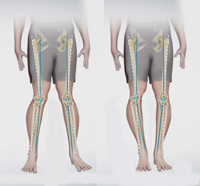 Knee Angular Deformities
Knee Angular Deformities
Procedures
Surgical Treatment
Knee Replacement and Reconstruction
-
 Unicompartmental Knee Replacement
Unicompartmental Knee Replacement -
 Patellofemoral Knee Replacement
Patellofemoral Knee Replacement - What is new in Knee Replacement
-
 Computer Navigation for Total Knee Replacement
Computer Navigation for Total Knee Replacement -
 Total Knee Replacement
Total Knee Replacement -
 Revision Knee Replacement
Revision Knee Replacement - Minimally Invasive Knee Joint Replacement
- Robotic Assisted Partial Knee Surgery
- Outpatient Total Knee Replacement
- After Knee Replacement